













Poster accepted and presented at the Alzheimer’s Association International Conference, 2019
Pathways
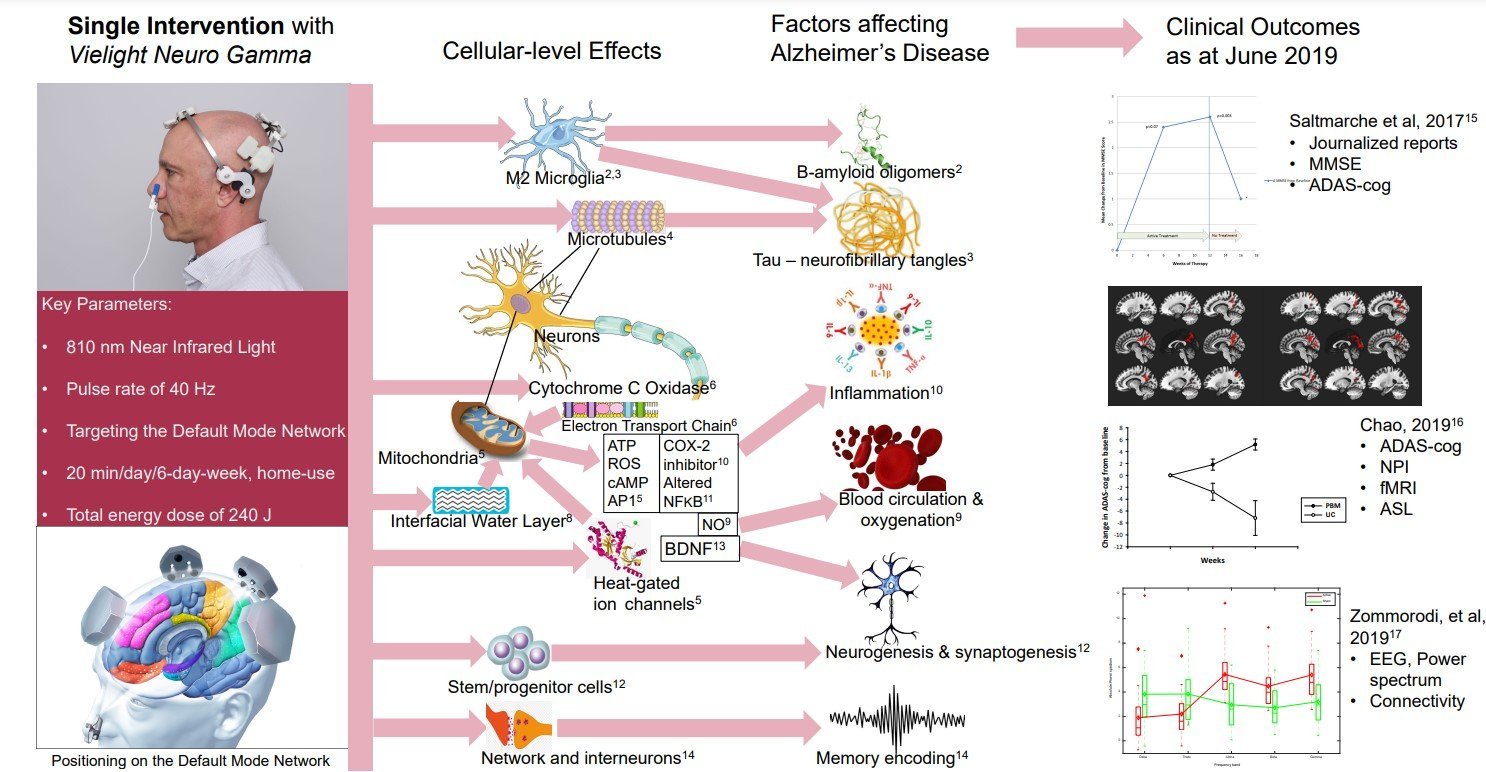
Photobiomodulation (PBM) in this presentation concerns the delivery of near infrared (NIR) to the brain to treat Alzheimer’s Disease (AD) using a home-use device, the Vielight Neuro Gamma. The key parameters are wavelength of 810 nm, pulse rate of 40 Hz, targeting the default mode network (DMN) for 20 minutes, delivering a total of 240 J. A similar device is in a pivotal trial expected to complete in 20211.
Recent animal research on flickering light at 40 Hz processed by brain areas have shown significant reduction in β-amyloid deposits through the activity of microglia2, presumably of the M2 non-inflammatory phenotype. Positive effect is also found for a tauopathy animal model3.
Microtubules provide the structure for the neuronal cytoskeleton. Their disintegration from tau protein abnormalities lead to neurofibrillary tangles. It has been found that the centrosomes in microtubules are able to detect NIR at 700-900 nm4 leading to discussion that there are positive implications for AD.
Much of PBM mechanism discussions have centered around the activity of the mitochondria which are numerous in eukaryotic cells such as neurons. The process produces key signaling molecules in adenosine triphosphate (ATP), low-level reactive oxygen species (ROS), cyclic adenosine monophosphate (cAMP) and activator protein-1 (AP1)5. An enzyme in the mitochondria membrane, cytochrome c oxidase, is considered a major chromophore for NIR photons6, acting as a photo-acceptor and signal transducer7. Calcium ion gated channels are directly activated by shorter wavelengths (blue) and longer IR wavelength activate a transient receptor potential (TRP) to activate the calcium channels5. NIR can also reduce the viscosity of Interfacial water layer, increasing ATP and cell proliferation8. PBM releases nitric oxide (NO) from the respiratory chain, activating vasodilatation, improving blood circulation and oxygenation9. Red light irradiation is found to be anti-inflammatory through the inhibition of the cyclo-oxygenase 2 (COX-2) enzyme by decreasing intracellular ROS10, and also altering NFKB activity11. Mice with brain injury treated with PBM increase progenitor cells in the dentate gyrus and in the sub-ventricular zone12. PBM has been shown to support the brain derived neurotrophic factor (BDNF) pathway, thus positively affecting dendritic morphogenesis and improved neuronal connectivity13. The presence of endogenous gamma oscillations has been found to correlate with higher quality memory encoding through interneuron and network-level activities14. PBM has also been associated with producing stem and progenitor cells that can develop into new T-cells to attack pathogens, a relatively new discovery in AD research.18
Outcomes
One of the first human trials of PBM for AD was reported by Saltmarche et al who treated a case series of five patients diagnosed with mild to moderately severe dementia with an early version of the Vielight Neuro. Functional and behavioral improvements were journalized and cognitive improvements were measured in MMSE and ADAS-cog scores15.
Chao published a pilot trial testing the effects of home PBM on cognitive and behavioral function, cerebral perfusion, and resting-state functional connectivity in eight patients (four PBM and four usual care) diagnosed with dementia. Significant improvements were observed in all the participants on real devices, measure in ADAS-cog scale, supported by fMRI and ASL imaging16.
A controlled study on healthy participants showed that inducing the parameters of the Vielight Neuro Gamma on healthy brains increases the power spectrum of the higher brain oscillatory frequencies, alpha, beta and gamma, and reduces those of the slower frequencies of delta and theta17.
References
- gov. Neuro RX Gamma – Pivotal Phase. Accessed July 2019: https://clinicaltrials.gov/ct2/show/NCT03484143.
- Iaccarino HF, Singer AC, Martorell AJ et al. Gamma frequency entrainment attenuates amyloid load and modifies microglia. Nature. 2016;540(7632):230-235.
- Adaikkan C, Middleton S.J, Marco A, et al. Gamma Entrainment Binds Higher-Order Brain Regions and Offers Neuroprotection. Neuron 2019; 102:929–943.
- Albrecht-Buehler G. Cellular infrared detector appears to be contained in the centrosome. Cell Motil Cytoskeleton. 1994;27(3):262-71.
- Hamblin, M.R. Photobiomodulation for Alzheimer’s Disease: Has the Light Dawned? Photonics 2019; 6:77.
- Cooper CE, Cope M, Springett R, et al. Use of Mitochondrial Inhibitors to Demonstrate That Cytochrome Oxidase Near-Infrared Spectroscopy Can Measure Mitochondrial Dysfunction Noninvasively in the Brain. Br. J. Pharmacol. 1999; 19:27–38.
- Karu TI. Multiple roles of cytochrome c oxidase in mammalian cells under action of red and IR-A radiation. IUBMB Life. 2010; 62:607–610.
- Sommer AP. Mitochondrial cytochrome c oxidase is not the primary acceptor for near infrared light—It is mitochondrial bound water: The principles of low-level light therapy. Ann. Transl. Med. 2019 7:S13.
- Lee HI, Lee SW, Kim SY, et al. Pretreatment with light-emitting diode therapy reduces ischemic brain injury in mice through endothelial nitric oxide synthase-dependent mechanisms. Biochem. Biophys. Res. Commun. 2017; 486:945–950.
- Lim W, Kim J, Kim S, et al. Modulation of lipopolysaccharide-induced NF-kappaB signaling pathway by 635 nm irradiation via heat shock protein 27 in human gingival fibroblast cells. Photochem. Photobiol. 2013; 89:199–207.
- Yamaura M, Yao M, Yaroslavsky I, et al. Low level light effects on inflammatory cytokine production by rheumatoid arthritis synoviocytes. Lasers Surg. Med. 2009; 41:282–290.
- Xuan W, Vatansever F, Huang L., et al. Transcranial low-level laser therapy enhances learning, memory, and neuroprogenitor cells after traumatic brain injury in mice. J. Biomed. Opt. 2014; 19:108003.
- Meng C, He Z and Xing D. Low-Level Laser Therapy Rescues Dendrite Atrophy via Upregulating BDNF Expression: Implications for Alzheimer’s Disease. J. Neurosci. 2013; 33:13505–13517.
- Palop JJ, Mucke L. Network abnormalities and interneuron dysfunction in Alzheimer disease. Nat Rev Neurosci. 2016; 17(12):777-792.
- Saltmarche AE, Naeser MA, Ho KF, et al Significant Improvement in Cognition in Mild to Moderately Severe Dementia Cases Treated with Transcranial Plus Intranasal Photobiomodulation: Case Series Report. Photomed. Laser Surg. 2017;35:432–441.
- Chao LL. Effects of Home Photobiomodulation Treatments on Cognitive and Behavioral Function, Cerebral Perfusion, and Resting-State Functional Connectivity in Patients with Dementia: A Pilot Trial. Photobiomodul. Photomed. Laser Surg. 2019; 37:133–141.
- Zomorrodi R, Loheswaran G, Pushparaj A & Lim L. Pulsed Near Infrared Transcranial and Intranasal Photobiomodulation Significantly Modulates Neural Oscillations: a pilot exploratory study. Scientific Reports. 2019; 9:6309.
- Dominy SS, Lynch C, Ermini F, et al. Porphyromonas gingivalis in Alzheimer’s disease brains: Evidence for disease causation and treatment with small-molecule inhibitors. Science Advances 2019;5:1.






Hello,
Can you please tell us when this trial is scheduled for completion?
May I join the study
1. What are the actual differences (e.g. more power, etc.) between the Neuro RX Gamma (used in the clinical trials) vs the Neuro GAMMA and APLHA, and will the non RX versions deliver similar results?
2. Since the results of the trials will be used to improve the efficacy of the Vielight devices, this infers that the current models may be changed over time to deliver better results. If this happens, will Vielight exchange the out of date versions for the newer more effective versions?
3. Are there any current plans to update the current versions in the near future, i.e. a roadmap for these devices?
Hi Linda,
Please reach out to us directly, as one of the criteria is the proximity to one of the study sites. We would need to know where you are located, and if there is a study site nearby, then you can be considered as a study subject.
Hello Tom,
Thank you for your interest and your questions. Please see replies below:
1. There is no difference between the Neuro Gamma and Neuro RX Gamma in terms of the output or any other factor that could affect efficacy of the devices. The differences are only relevant to the special regulatory guidelines for the devices used in a trial, and they are not affecting the performance of the device.
2. The results of the study will show whether the devices provide sufficient efficacy to be considered medical devices. If that will be the case, no changes to these devices will be made.
3. We are always working on something new and will make relevant announcements in due course as appropriate.
My husband has AD and we have been using the Vie Light for approximately 12 weeks, 6 times a week. At the end of the 12 weeks, we will go to either 3 times a week or every other day depending on what I can learn from any additional research. Can you direct me to any other research that specifically addressed the number of times per week the person used the devices?
I have been keeping a journal throughout the time we’ve been using the devices, and I will share what we’ve learned soon.
Thank you.
Bev. Santo